
Hip dysplasia is a fairly common condition in both adolescents and adults. It ranges from being a barely detectable issue to a severe malformation that causes extreme pain and disruption to daily life. The following is basic yet important information to know in the event that you or family members are affected by this condition.
Hip anatomy
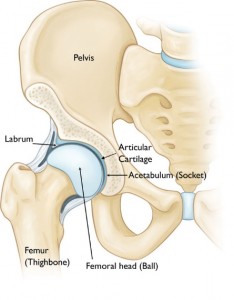
The hip joint is a ball and socket joint. The upper part of the femur (thighbone) has an angled neck and a round head (the ball). The bones of the pelvis come together to form the acetabulum (the socket). The head of the femur and the acetabulum are both covered with articular cartilage—a rubbery, lubricated, low friction-bearing surface that allows for smooth and painless joint motion. Around the rim of the acetabulum, there is a ring of dense fibrocartilage that forms a suction seal around the joint; this ring is called the labrum.
What is hip dysplasia?
Dysplasia refers to a condition where the hip joint is abnormally formed in early development. The condition can affect the thighbone, causing abnormalities in the angle and rotation of the upper part of this bone. However the most common and most notable findings in hip dysplasia are those pertaining to the socket. Dysplastic hips are characterized by abnormally shallow sockets, as seen below.

Example of hip joints with shallow sockets
The result is that the area of contact between the ball and socket is decreased. This decrease in contact area results in an increase in pressure on the articular cartilage in the joint. Over time, this can lead to pain and progressive damage to the labrum and articular cartilage. Ultimately, if left untreated, significant dysplasia is associated with the development of hip arthritis at a young age.
When does dysplasia occur?
Dysplasia has been called Congenital Hip Dysplasia (present from birth) and also Developmental Dysplasia of the Hip (occurring during hip development) because the abnormality is generally present to some extent at birth but can change and evolve as the hip joint grows and matures.
Adolescence and adulthood
Whether the dysplasia was mild enough in childhood so that it was never diagnosed or was diagnosed and treated with harness, bracing, and/or surgery, the dysplastic hip can, in some cases, remain an issue in adolescence and adulthood. The hip joint continues to grow, develop and change as long as the bones are growing. Early treatments with harness or bracing aim to guide the development of the hip into a more natural shape. Once bone growth stops, a time referred to as skeletal maturity, the hip joint ceases to develop further and the degree of dysplasia that is present will persist.
Measuring dysplasia
Various measurements have been described to define the severity of dysplasia in the skeletally mature hip. Physicians use these measurements to understand the degree of the dysplasia and to guide recommendations for treatment. The most commonly utilized measurements include the Tӧnnis angle and the Lateral Center Edge Angle.

Lateral Center Edge angle
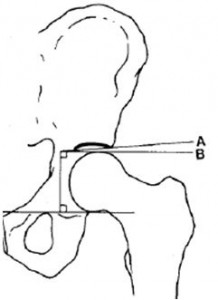
Tӧnnis angle
The Tӧnnis angle (right) measures the slope of the roof of the acetabulum. In a normal hip this should be relatively flat—less than 11 degrees.
The Lateral Center Edge angle (far right) is a means to estimate how much of the femoral head is covered by the socket. Normal values are greater than 25 degrees. Angles between 20 and 25 degrees are considered mild or borderline dysplasia. Values less than 20 indicate more severe dysplasia.
Symptoms of hip dysplasia
In adolescents and adults, dysplasia is most commonly manifested as activity-related hip pain and, occasionally, a limp. The causes of pain in the dysplastic hip may include:
- Muscle fatigue: The muscles surrounding the hip joint, in particular the hip abductor muscles, tend to work overtime in the dysplastic hip in order to keep the hip firmly seated in the shallow socket at all times. Patients with hip dysplasia may note soreness on the sides of the hip with prolonged standing or walking.
- Labral injury: The labrum can be damaged by shear stress at the rim of the socket causing it to pull away from the rim. This can cause a feeling of groin pain, which may be exacerbated by certain maneuvers or extremes of hip range of motion.
- Articular cartilage damage: The increased contact pressure in the dysplastic hip can, over time, lead to progressive damage to the articular cartilage and, if left uncorrected, can eventually result in the development of hip arthritis at an early age.
Treating the skeletally mature dysplastic hip
The treatment of dysplasia in the skeletally mature hip is no longer focused on guiding growth and development. The goals of treatment in this case are to:
- Optimize the function of the hip joint
- Alleviate pain resulting from a shallow socket
- Prolong the use of the native hip joint and avoid hip replacement at a young age
In milder cases, these goals can sometimes be achieved with physical therapy. This will not change the shape of the hip joint or eliminate the dysplasia. However, if the dysplasia is relatively mild, strengthening the muscles around the hip joint can have a positive effect on hip function.
In more severe cases, treatment of dysplasia is geared towards the correction of the underlying anatomic abnormality. This is achieved by cutting and moving the bones into more proper alignment. When a bone is cut and moved to change its shape, this is referred to as an osteotomy.
Surgical treatments for hip dysplasia can include an osteotomy around the acetabulum, also called a periacetabular osteotomy and/or an osteotomy of the femur (femoral osteotomy). The goals of these procedures are to correct the abnormal shape of the hip joint, which can reduce the pain related to hip dysplasia and may reduce the risk of developing early arthritis.
Hip dysplasia and arthritis
In some cases hip dysplasia, whether diagnosed and treated or not, will result in significant damage to the articular cartilage. When the articular cartilage begins to wear out, this is known as hip arthritis. Once a hip has significant arthritis, it may no longer be possible to preserve the native hip joint. In this case hip replacement is the most reliable option to relieve pain and restore function.
 Dr. Benjamin McArthur is a fellowship-trained orthopaedic surgeon with specializations in hip and knee replacement, complex revision hip and knee replacement, and hip preservation surgery. He has published numerous peer-reviewed articles and has presented at national and international events on topics related to hip and knee replacement. He is a reviewer of current research for the Bone and Joint Journal, The Journal of Arthroplasty, and the American Journal of Orthopedics.
Dr. Benjamin McArthur is a fellowship-trained orthopaedic surgeon with specializations in hip and knee replacement, complex revision hip and knee replacement, and hip preservation surgery. He has published numerous peer-reviewed articles and has presented at national and international events on topics related to hip and knee replacement. He is a reviewer of current research for the Bone and Joint Journal, The Journal of Arthroplasty, and the American Journal of Orthopedics.
Additional patient resources:
http://orthoinfo.aaos.org/topic.cfm?topic=A00347
http://orthoinfo.aaos.org/topic.cfm?topic=A00710
http://hipdysplasia.org/adult-hip-dysplasia/
Want to know more?
For more information about hip dysplasia, email us or request an appointment.
Be sure to follow us on Facebook and Twitter as well!