
“Hey doc, I’m worried I have carpal tunnel syndrome.”
I hear this almost every day in the office. Everybody has heard of carpal tunnel syndrome (CTS) and many people assume that all wrist and hand pain is caused by CTS. But CTS is a very specific condition that results in very specific symptoms.
Carpal tunnel syndrome is caused by compression of the median nerve in a confined space in the wrist we call the carpal tunnel and is the most common compression neuropathy. The median nerve is the nerve that generally provides sensation or feeling to the thumb, index finger, middle finger, and one half of the ring finger. It also provides the motor input to some of the muscles of the thumb called the thenar muscles.

Area of sensation of the median nerve
What are the symptoms of carpal tunnel syndrome?
Patients with CTS complain of:
- Numbness and tingling in their hand, specifically in the thumb, index finger, middle finger, and half of the ring finger.
- Numbness and tingling that often starts at night or with activities that involve gripping and grasping, such as driving a car, reading a book, or biking.
- Weakened grip, trouble fastening buttons, or performing other fine motor activities.
- These symptoms can wax and wane depending on the patient’s activities but generally get worse over time.
How do we diagnose carpal tunnel syndrome?
We make the diagnosis of CTS by a taking a history and examining the patient. The history includes the identification of symptoms and what makes them better or worse, any associated medical conditions, and hobbies and activities. The physical exam includes a general exam of the neck and arms as well as special tests specific to CTS. Depending on the circumstances, we may also recommend a nerve test called EMG/ NCV (electromyography/nerve conduction velocity) to help confirm the diagnosis.
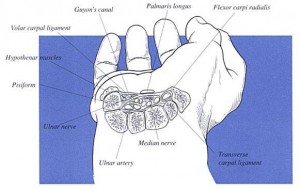
The carpal tunnel
Other conditions that can cause similar symptoms to CTS include peripheral neuropathy, cervical disc disease, and other neurologic conditions. Other causes of hand pain include tendinitis, arthritis, and other nerve issues.
Who gets carpal tunnel syndrome?
CTS is extremely common. There are a number of risk factors that predispose one to developing CTS. First of all, there is probably a genetic component. Women are more likely to develop CTS than men, particularly peri-menopausal women. Hypothyroidism, pregnancy, obesity, and inflammatory conditions such as rheumatoid arthritis, are also known risk factors. Trauma from a fracture or significant injury to the hand or wrist may play a role in the development of CTS. Finally, repetitive forceful gripping, such as using power tools, is also believed to contribute to the development of CTS.
How do we treat carpal tunnel syndrome?
CTS treatment depends on the severity of the symptoms and the physical findings. We generally start with a trial of splinting the wrist at night and activity modification. Occasionally, anti-inflammatory medications such as Motrin or Aleve may be prescribed. A brief course of occupational therapy can also be helpful. Patients will often respond to conservative treatment. Patients who don’t improve with conservative treatment may be offered a steroid injection into the carpal tunnel that may provide long term relief. Finally, patients with unremitting or severe symptoms may be offered a surgical option.

Significant atrophy of thenar muscles seen in severe CTS
Surgery
If surgery for CTS is recommended, it can be performed with different techniques.
The first approach is the small incision open technique. This is done as an outpatient and generally is performed under local anesthesia. Some patients prefer “twilight anesthesia” to local anesthesia, which can be accommodated. A one-inch incision is made in the palm and the transverse carpal ligament is released. Following the surgery, a small dressing is applied and patients can resume light activities immediately, including typing and eating. There is a restriction on heavy lifting for 3 weeks although some patients are a little too sore to resume unrestricted activities such as golf, biking, and tennis until 4–12 weeks after surgery and rarely longer.
The other option is the endoscopic technique. Endoscopic carpal tunnel release in generally performed with light sedation and by numbing the arm. Through a small incision at the junction of the wrist and the forearm, an endoscope is inserted and the transverse carpal ligament is released. Similar to the small incision open technique, a light dressing is applied and the patient may resume light activities immediately and unrestricted activities at 3 weeks after the surgery. Some patients may be too sore to resume all activities until 4–6 weeks after the surgery and sometimes longer.

Intact transverse carpal ligament
Pros and cons
There are pros and cons to each approach and your surgeon can discuss them with you. The major advantage to the endoscopic technique is a faster return to unrestricted activities in people who are very active. One could expect a quicker return to heavy labor and sports such as golf, tennis, biking, and weight lifting. The major advantage of the small incision open technique is that it can be done under local anesthesia, which is beneficial to patients who have significant risk factors for more involved anesthesia.

Cut transverse carpal ligament
What to expect after surgery
CTS surgery has a success rate in the high 90 percent range. Most patients experience immediate relief of the night symptoms and a quick return to light use after the surgery. Many patients return to unrestricted activities 3–6 weeks after the surgery, although it can sometimes take months to be completely pain-free and for strength to return to normal. However, there are two reasons some patients do poorly.
The first is that they did not have CTS or there was another problem, such as neuropathy, nerve compression in the neck, or nerve compression elsewhere in the arm. This can be avoided with a careful history and physical exam and nerve studies when appropriate. The second, and probably the most common reason, is that the CTS was already so severe that the nerve was beyond recovery. The latter can be avoided by proceeding with surgery in a timely fashion before the nerve is permanently damaged.
Conclusion
While CTS is a common condition, if left undiagnosed or untreated, it can severely impact your daily life and even your job. A hand and wrist specialist can determine if the pain or weakness you’re experiencing is CTS and prescribe the appropriate course of action to take for treatment.

Dr. Richard W. Barth is a board-certified orthopaedic surgeon at Washington Orthopaedics & Sports Medicine. He specializes in surgery of the hand and upper extremity, particularly upper extremity sports injuries. Dr. Barth has served as a hand and wrist consultant for the Washington Capitals and Washington Wizards and is a former president of the Washington Orthopaedic Society. He is an associate clinical professor of Orthopaedics at George Washington University and is chief of Orthopaedic Surgery/Hand Surgery and vice chairman of the Department of Surgery at Sibley Memorial Hospital.
Want to know more?
For more information about carpal tunnel syndrome, email us or request an appointment.
Be sure to follow us on Facebook and Twitter as well!