
What is a partial knee replacement?
A partial knee replacement, also called unicompartmental knee arthroplasty, or UKA, is a surgery that aims to resurface only the arthritic or damaged portion of the knee joint.
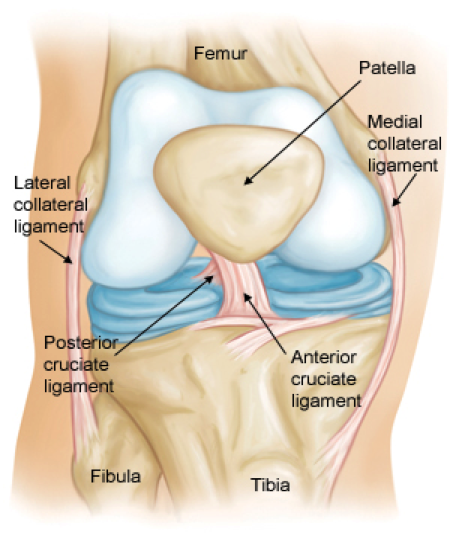
Anatomy:
The inside of the knee can be divided into three main articulations or joint surfaces known as compartments (visualizations of these can be seen in the “Uni Knee Replacement” video here). The medial and lateral (tibiofemoral) compartments contain the joint surfaces between the bones of the thigh (femur) and the lower leg (tibia), and the patellofemoral compartment is the joint surface between the femur and the knee cap (patella). In each of these joint spaces, the ends of the bones are covered with articular cartilage, which, when healthy, is a rubbery, lubricated, low friction surface that allows smooth and painless motion in the joint. When the articular cartilage starts to degenerate or break down, arthritis develops.

Arthritis is commonly found in the medial compartment
The most common area for arthritis development is the medial compartment; thus medial unicompartmental knee arthroplasty is the most common partial knee replacement performed.
Studies comparing knee motion both in live subjects and in cadaver models have confirmed that subtle changes in knee rotation during flexion are much more similar when comparing a native knee to a partial knee replacement as opposed to a total knee replacement.
Why was partial knee replacement developed?
The classic treatment for advanced knee arthritis, when the cartilage is severely damaged or absent, and non-surgical treatments are no longer effective, has been total knee replacement. Total knee replacement resurfaces all three compartments in the knee and thus largely eliminates pain related to knee arthritis. This has been a highly effective operation and has helped millions of people regain mobility and dramatically improve knee function.
However, there is room for improvement. While the majority of people do very well after total knee replacement, multiple studies have shown that some percentage of patients, between 11-19% in fact, may be dissatisfied with the results1-9. Common reasons cited for dissatisfaction include failure to meet expectations in terms of the feel and function of the knee or the occurrence of a complication requiring re-admission to the hospital.
The goals of partial knee replacement were to develop a less invasive, more natural feeling knee, while at the same time reducing the stress of surgery and the incidence of post-operative complications.
How does partial knee replacement compare to total knee replacement?
So how do partial knee procedures measure up to total knee procedures in practice? As with any therapy, there are advantages and disadvantages to each option and both need to be carefully considered when determining if partial knee replacement is a reasonable option for you.
Advantages
Less invasive surgery
Since only one compartment of the knee is being replaced, the surgical procedure is less extensive. The term “minimally invasive” or “less invasive” is used frequently but can be ill-defined. In the case of partial versus total knee replacement surgery, the specific differences that have been demonstrated in several published studies include:
- A smaller incision. Typically a partial knee replacement can be done with an incision about half as long as the standard total knee replacement incision.
- Less soft tissue dissection. Since only one area of the knee needs to be fully accessed, partial knee replacement typically involves less disruption of the native anatomy to gain access for surgery. The quadriceps tendon in particular is typically not violated or disrupted during exposure for a partial knee replacement.
- Less bleeding. The smaller exposure has been shown consistently to reduce bleeding at the time of surgery, which has obvious benefits in terms of the physiologic impact of surgery and ease of recovery.
As a result, partial knee replacement has been associated with less pain and fewer complications around the time of surgery (such as blood clots, need for transfusion, and surgical site infection).
Rapid recovery
A number of studies have shown quicker recovery after partial knee replacement both in terms of time spent in the hospital and also time required to meet functional goals. Time spent in the hospital after surgery is variable but, on average, patients spend 2–3 nights in the hospital after a routine total knee replacement. After a partial knee replacement, patients often go home the same day or spend only one night in the hospital.
Studies assessing return to function have also shown a significant difference between total and partial knee replacements. One study compared minimally invasive partial knee replacement to total knee replacement with regard to the time required for patients to achieve independent stair climbing, straight leg raise, and flexion to 70 degrees10. The authors noted that patients achieved these goals three times faster after partial knee replacement than after total knee replacement.
More natural knee motion
Partial knee replacements have been found to have improved knee kinematics compared to total knee replacements. This means that knees with a partial replacement move more like a natural knee. One major reason for this is that partial knee replacement does not require sacrifice of any of the native knee ligaments.
Partial knee replacement preserves the cruciate ligaments
In contrast, a routine total knee replacement typically involves removing one or both of the cruciate ligaments in the center of the knee. These ligaments are preserved in partial knee replacement and have a significant impact on the way that the knee moves. The result is that a partial knee replacement moves and feels more like a natural knee.
Studies comparing knee motion both in live subjects and in cadaver models have confirmed that subtle changes in knee rotation during flexion are much more similar when comparing a native knee to a partial knee replacement as opposed to a total knee replacement11,12. Patients have also been shown to have better knee range of motion on average after partial knee replacement compared to total knee replacement10,13. Furthermore, patients who have had a total knee replacement on one knee and a partial knee replacement on the other knee tend to report that the partial knee replacement feels more natural14.
Potential Problems
Progression of arthritis
Naturally, since the concept behind partial knee replacement is to only replace one compartment out of three, there is a risk of developing arthritis in other areas of the knee. If some degree of arthritis is obvious in more than one compartment of the knee, the risk of developing painful arthritis in other areas of the knee may be too high for a partial knee replacement to be a reasonable option. Special x-rays known as stress views can be helpful in determining if there is significant arthritis in areas that appear to be unaffected. Even in cases where arthritis is clearly confined to a single compartment, it is possible for arthritis to later develop, which may require subsequent conversion to a total knee replacement
Loosening of the implant
Because the implants used for partial knee replacement are smaller than total knee implants and require meticulous technique in their insertion, early studies reported higher rates of implant loosening after partial replacement than total replacement. However modern implant designs and evolution in surgical technique have led to significant improvements in long-term outcomes after partial knee replacement, with studies demonstrating over 90% of implants remain in place at 10 years and over 80% remain in place at 20 years15-18.
Survivorship
A direct comparison of survivorship, meaning how long an implant remains in place without having to be revised or changed, demonstrates a slight advantage for total knee replacement. Statistics from a large Australian database revealed that at 10 years, the probability of survivorship for a partial knee replacement was 0.9 times the probability of a total knee replacement19.
Who is a good candidate for Partial Knee Replacement?
Good candidates for partial knee replacements should have:
- Arthritis isolated to a single compartment of the knee
- Intact knee ligaments
- No significant fixed deformity of the knee
Activity level after Partial Knee Replacement
While early studies suggested that partial knee replacement should be reserved for elderly and more sedentary patients, recently a number of studies have noted excellent outcomes in younger, more active patients20. Furthermore, as younger, more active patients are undergoing partial knee replacement, patient goals and expectations are changing. Rather than living a sedentary lifestyle after surgery, one studied noted that 83.4% of patients had resumed sports after partial knee and 90% of patients reported that they felt little or no limitations in their athletic activities21.
How do I know if Partial Knee Replacement is right for me?
Pre-operative assessment
The decision to consider partial knee replacement should be based on a thorough history and physical exam carried out by your surgeon and a careful review of the knee X-ray, including a stress view when indicated.
Intra-operative decision
Though every effort is made to determine if a patient is a good candidate before the day of surgery, the final decision to proceed with a partial replacement needs to be made in the operating room once the surgery is underway. A quick look at the cartilage in the other compartments of the knee joint, along with an assessment of the cruciate ligaments, should take place prior to proceeding with partial knee replacement. If significant damage is noted, a total knee replacement can be done instead.
Summary
- Partial Knee Replacement is a safe and effective treatment option for the patient with:
- unicompartmental arthritis
- intact ligaments
- correctable deformity
- In appropriately selected patients, partial replacement may offer several benefits over total knee replacement with regards to recovery and functional outcome.
- Careful patient selection is critical to ensure the best possible survivorship.
 Dr. Benjamin McArthur is a fellowship-trained orthopaedic surgeon with specializations in hip and knee replacement, complex revision hip and knee replacement, and hip preservation surgery. He has published numerous peer reviewed articles and has presented at national and international events on topics related to hip and knee replacement. He is a reviewer of current research for the Bone and Joint Journal, Clinical Orthopedics and Related Research, and the Journal of the Hospital for Special Surgery.
Dr. Benjamin McArthur is a fellowship-trained orthopaedic surgeon with specializations in hip and knee replacement, complex revision hip and knee replacement, and hip preservation surgery. He has published numerous peer reviewed articles and has presented at national and international events on topics related to hip and knee replacement. He is a reviewer of current research for the Bone and Joint Journal, Clinical Orthopedics and Related Research, and the Journal of the Hospital for Special Surgery.
Want to know more?
For more information about partial knee replacements, email us or request an appointment.
Be sure to follow us on Facebook and Twitter as well!
References:
- Anderson JG, Wixson RL, Tsai D, Stulberg SD, Chang RW. Functional outcome and patient satisfaction in total knee patients over the age of 75. J Arthroplasty. 1996;11:831–840.
- Chesworth BM, Mahomed NN, Bourne RB, Davis AM. Willingness to go through surgery again validated the WOMAC clinically important difference from THR/TKR surgery. J Clin Epidemiol. 2008;61:907–918.
- Dunbar MJ, Robertsson O, Ryd L, Lidgren L. Appropriate questionnaires for knee arthroplasty. Results of a survey of 3600 patients from the Swedish Knee Arthroplasty Registry. J Bone Joint Surg Br. 2001;83:339–344.
- Hawker G, Wright J, Coyte P, Paul J, Dittus R, Croxford R, Katz B, Bombardier C, Heck D, Freund D. Health-related quality of life after knee replacement. Results of the knee replacement patient outcomes research team study. J Bone Joint Surg Am. 1998;80:163–173
- Heck DA, Robinson RL, Partridge CM, Lubitz RM, Freund DA. Patient outcomes after knee replacement. Clin Orthop Relat Res. 1998;356:93–110
- Noble PC, Conditt MA, Cook KF, Mathis KB. The John Insall Award: Patient expectations affect satisfaction with total knee arthroplasty. Clin Orthop Relat Res. 2006;452:35–43
- Robertsson O, Dunbar M, Pehrsson T, Knutson K, Lidgren L.Patient satisfaction after knee arthroplasty: a report on 27,372 knees operated on between 1981 and 1995 in Sweden. Acta Orthop Scand. 2000;71:262–267
- Wylde V, Learmonth I, Potter A, Bettinson K, Lingard E. Patient reported outcomes after fixed- versus mobile-bearing total knee replacement: a multi-centre randomised controlled trial using the Kinemax total knee replacement. J Bone Joint Surg Br. 2008;90:1172–1179
- Bourne RB, Chesworth BM, Davis AM, Mahomed NN, Charron KD. Patient satisfaction after total knee arthroplasty: who is satisfied and who is not? Clin Orthop Relat Res. 2010 Jan;468(1):57-63
- Price AJ, Webb J, Topf H, Dodd CA, Goodfellow JW, Murray DW; Oxford Hip and Knee Group. Rapid recovery after oxford unicompartmental arthroplasty through a short incision. J Arthroplasty. 2001 Dec;16(8):970-6
- Patil S, Colwell CW Jr, Ezzet KA, D’Lima DD. Can normal knee kinematics be restored with unicompartmental knee replacement? J Bone Joint Surg Am. 2005 Feb;87(2):332-8
- Robinson BJ, Rees JL, Price AJ, Beard DJ, Murray DM; OHKG. Oxford Hip and Knee Group. A kinematic study of lateral unicompartmental arthroplasty. Knee. 2002 Sep;9(3):237-40
- Newman J, Pydisetty RV, Ackroyd C: Unicompartmental or total knee replacement: the 15- year results of a prospective randomised controlled trial. J Bone Joint Surg Br. 2009; 91:52
- Laurencin CT, Zelicof SB, Scott RD,Ewald FC: Unicompartmental versus total knee arthroplasty in the same patient: A comparative study. Clin Orthop Relat Res 1991;273:151-156
- Murray DW, Goodfellow JW, O’Connor JJ. The Oxford medial unicompartmental arthroplasty: a ten-year survival study. J Bone Joint Surg Br. 1998 Nov;80(6):983-9.
- Berger RA, Meneghini RM, Jacobs JJ, Sheinkop MB, Della Valle CJ, Rosenberg AG, Galante JO. Results of unicompartmental knee arthroplasty at a minimum of ten years of follow-up. J Bone Joint Surg Am. 2005 May;87(5):999-1006
- Squire MW, Callaghan JJ, Goetz DD, Sullivan PM, Johnston RC. Unicompartmental knee replacement. A minimum 15 year followup study. Clin Orthop Relat Res. 1999 Oct;(367):61-72.
- Svärd UC, Price AJ. Oxford medial unicompartmental knee arthroplasty: a survival analysis of an independent series. J Bone Joint Surg Br 2001;83(2):191–4.
- AOANJR (Australian Orthopaedic Association National Joint Replacement Registry)
- Price AJ, Dodd CA, Svard UG, Murray DW. Oxford medial unicompartmental knee arthroplasty in patients younger and older than 60 years of age. J Bone Joint Surg Br. 2005 Nov;87(11):1488-92
- Felts E, Parratte S, Pauly V, Aubaniac JM, Argenson JN. Function and quality of life following medial unicompartmental knee arthroplasty in patients 60 years of age or younger. Orthop Traumatol Surg Res. 2010 Dec;96(8):861-7