
Proper diagnosis and treatment are key to avoid future problems
Growth plate fractures are very common in children. Approximately 15–30% of all childhood fractures occur through the growth plate. They are twice as likely to occur in boys as in girls.
The most common locations for growth plate fractures are the wrist and elbow, followed by the ankle, knee, and hip. Growth plate fractures often need immediate treatment because they can affect how the bone will grow. Improper treatment can lead to crooked or shortened limbs.
What is a Growth Plate?
A growth plate, also known as the epiphyseal plate or physis, is an area of cartilage tissue near the ends of long bones in children and adolescents. As children grow, the cartilage turns into bone and determines the length and shape of the mature bone. Similar to bone, an injury to the growth plate is also known as a fracture. Growth plates are weaker than the bone and nearby ligaments and tendons. This is why children are more likely to fracture their ankles and wrists rather than sprain them like adults.
On the outside of the growth plate, young cartilage cells, known as chondrocytes, are continuously dividing. The new cells stack on top of one another, facing the outer portion of the long bone (the epiphysis) while the older cells are pushed inward toward the shaft of the long bone (the diaphysis) where they become mature bone cells. Estrogen levels increase during puberty (for both boys and girls) and cause ossification to accelerate until the cartilage is completely replaced by bone. Girls often stop growing two or three years after their menses, while boys might not stop growing until they are 18–21.
Causes
Fractures can occur from one traumatic event or from repetitive overuse. Traumatic events are wide ranged and include something as simple as falling off a bicycle to more extreme cases, like a car accident. With every step or muscle action taken, we are breaking down our bones. However, the cells that build them back up work 150 times slower—and sometimes that can lead to overuse injuries, which include stress fractures.
Symptoms
 Children who have persistent pain, or pain that affects their athletic performance or ability to move and puts pressure on a limb, may get a possible fracture or overuse injury.
Children who have persistent pain, or pain that affects their athletic performance or ability to move and puts pressure on a limb, may get a possible fracture or overuse injury.
Once the patient is examined by a physician, an x-ray will be obtained. Many times a growth plate injury does not appear on an x-ray because the normal growth plate appears as a gap between the ossified bone, as seen below. With an adequate history and physical exam from skilled physicians, such as those at WOSM, a diagnosis can be made.
Growth Plate Fracture Classification
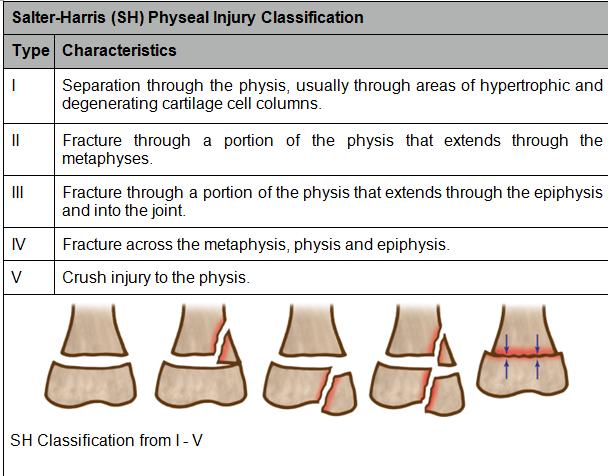
The Salter-Harris classification is the most widely used and accepted classification to describe these types of fractures. Almost all children with physeal injuries can be classified from plain x-rays using the Salter-Harris classifications. There are instances where the injury can be so complex that additional imaging may be helpful, including a CT or MRI.
There are five types of growth plate fractures. Type I and Type II are common at the wrist, ankle, knee, and shoulder.
Kliegman RM et Al. Nelson Essentials of Pediatrics. Saunders; 2007, p 2838
Treatment
If it is a simple fracture, most likely Salter-Harris types I and II, the physician will immobilize the injury with a cast or brace for approximately a month or longer. Once the injured limb is healed, the child can resume normal activities as tolerated. Sometimes children may require physical therapy, but most of the time they do not.
The bone will remodel itself using the remaining bone as its supporting architecture. The younger the child is, the better the remodeling potential. If the fracture is displaced, there could be a need for surgery in order to realign the bone and prevent growth disturbances. Exactly accurate reduction of the bone is critical at the ankle and knee because these are weight-bearing surfaces where pressures are the greatest. Type III and Type IV injuries involve the joint surface and therefore require anatomic reduction and often surgical stabilization.
Sometimes crush or high velocity injuries may result in early closure or fusion of a growth plate, which could lead to deformity and impaired function of the affected limb. The risk of growth problems is related to the amount of energy resulting in the fracture, the type of growth plate fracture, and the bone that is injured. The higher the energy that causes the fracture, the more likely the bone will stop growing. While your surgeon may try to align the growth plate as perfectly as possible, this does not guarantee that a growth problem can be avoided.
Seek help for constant pain
Overall, you should avoid trying to ignore persistent pain for more than a couple of days, as it may be indicative of a more severe injury rather than a simple sprain. Most growth plate injuries need 10–14 days to start uniting, making the reduction and fixation more difficult the longer treatment is delayed. Be sure to get help early.
Want to know more?
For more information about growth plate injuries, email us or request an appointment. Be sure to follow us on Facebook and Twitter as well!

Dr. Richard M. Grossman is a founding member of Washington Orthopaedics and Sports Medicine. He has served as team physician for the Washington Wizards, Washington Capitals, and the Georgetown University athletic program, and consults for the NFL Players Association as well as several independent school athletic programs in the Washington, D.C. area. He has been listed on Washingtonian Magazine’s Top Doctors list since its inception, and was named Bethesda Magazine’s Top Orthopedic Surgeon in 2008–2009.