
Dupuytren’s disease, or Dupuytren’s contracture, is a condition of the hand in which the fingers flex and contract, or permanently curl, into the palm. Dense nodules underneath the skin and pitting of the skin can also be present. The small finger and ring finger are most commonly affected, but any part of the hand can be involved.
As this disease progresses, it becomes more difficult to extend the fingers and flatten the hand, making simple tasks like shaking hands, washing one’s face, or even reaching into a pocket difficult, if not impossible. Usually Dupuytren’s disease is painless. Many patients believe the tendons are contracted but it is actually the structure between the tendons and the skin, called the palmar fascia, which is diseased; the tendons themselves are uninvolved.
Who was Guillaume Dupuytren?
 Dupuytren’s contracture is named after a famous French anatomist and military surgeon named Guillaume Dupuytren (1777–1835). Dupuytren was a medical prodigy. By age 20, he was appointed assistant surgeon at Paris’ Hôtel-Dieu. His ability to diagnose and heal others earned him great fame and fortune. In 1816, he was appointed head surgeon at Hôtel-Dieu, a position he held until his death.
Dupuytren’s contracture is named after a famous French anatomist and military surgeon named Guillaume Dupuytren (1777–1835). Dupuytren was a medical prodigy. By age 20, he was appointed assistant surgeon at Paris’ Hôtel-Dieu. His ability to diagnose and heal others earned him great fame and fortune. In 1816, he was appointed head surgeon at Hôtel-Dieu, a position he held until his death.
Interestingly, Dupuytren’s contracture was not originally described by Guillaume Dupuytren, but rather by the Swiss physician Felix Plater (1536-1614). Plater described this contracture of the hand in 1614, nearly 150 years prior to Dupuytren’s birth.[i]
Cause
Cells called myofibroblasts are responsible for the development of these contractures. Myofibroblasts reside within the tissue, just beneath the palmar skin, in a layer of tissue called “fascia” or “aponeurosis.”
Who gets Dupuytren’s disease?
Dupuytren’s disease is seen more frequently in men than in women (by a ratio of 7 to 1); in those over 60 years of age; and usually, but not exclusively, people with northern European, British, or Scandinavian ancestry. When women are affected, the disease progression is often atypical, and sometimes more severe. The gene for Dupuytren’s is inherited as an autosomal dominant trait. Many patients usually have someone in their family who also has Dupuytren’s.
Treatment and restoration of normal function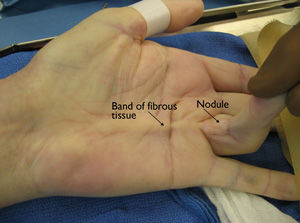
Dupuytren’s contracture is a complex condition that should only be treated by a trained hand specialist. With recent advances in technique and pharmacology, there are several options to consider when treating the disease.
Surgical treatment
Traditionally, Dupuytren’s contracture has been treated surgically by excising the cords and nodules in what is called a “palmar fasciectomy.” Technically, the surgery is very challenging, but results can be very good to excellent. The procedure is usually performed as outpatient surgery, and takes about 1 or 2 hours, depending upon the severity of the contracture. Afterwards, a splint is worn full time for 4 to 6 weeks, and then only at night for another 4 to 6 weeks. Hand therapy after this procedure is common. Patients usually have very limited use of the hand for several weeks following the surgery and may need a few months to return to unrestricted use.
Needle aponeurotomy (NA)
This is a newer, less invasive approach to treating Dupuytren’s contracture. This technique can be performed in the office or outpatient surgery center using local anesthesia. NA uses a small hypodermic needle to divide the palmar cords and straighten the finger. This procedure takes less than 30 minutes.
Afterwards, a splint or soft dressing may be applied, based upon your surgeon’s preference. The need for hand therapy after this procedure is variable, depending on your surgeon. Again, results can be excellent, and the procedure is quick and relatively inexpensive, and generally involves minimal pain for the patient.[i] Patients generally can return to light use of their hand, including typing and light gripping immediately after the procedure, and unrestricted use at 2 to 4 weeks.

Pre-procedure
Immediately after procedure

6 months later
Collagenase injections
The injection of collagenase is the latest technique in treating Dupuytren’s contracture, having gained FDA approval in 2010. Collagenase is a chemical that breaks down the collagen structure within the palmar cords. In the doctor’s office, collagenase is injected directly into the palmar cord. Over the next 24 hours the cord breaks down, and the patient returns to the doctor’s office in 24 to 48 hours for manipulation of the affected joint. Like NA, splinting and hand therapy depend upon your doctor’s preferences. Results can be excellent.[i]
DNA is the determinant
Because the proclivity for the hand to contract is “hard-wired” in the myofibroblast’s cellular DNA, the only way to truly eradicate Dupuytren’s disease would be to alter one’s genetic code. Until gene modification is achieved, the risk of recurrence at 3 to 5 years is high in all three of the above procedures. Comparative studies show that at 5 years, Dupuytren’s contracture treated surgically has a lower recurrence rate than if treated with either NA or collagenase.[ii]
Conclusion
Many patients with early Dupuytren’s disease require only reassurance that the lumps and bumps in their hand are not tumors and that observation is reasonable. An experienced hand surgeon can often make this determination by the history and physical exam, and a biopsy is rarely necessary. When indicated, surgical treatment, needle aponeurotomy, and collagenase injection each have specific risks and benefits. On an individual basis, the physician and the patient will determine which treatment option best fits the circumstances.
Washington Orthopaedics & Sports Medicine has extensive experience with Dupuytren’s disease, all three treatment methods, and other hand and upper extremity conditions. If you think you have Dupuytren’s contracture, please call the hand specialists at WOSM to schedule an office examination.
Want to know more?
For more information about Dupuytren’s contracture, email us or request an appointment.
 Dr. Richard W. Barth is a board-certified orthopaedic surgeon at Washington Orthopaedics & Sports Medicine. He specializes in surgery of the hand and upper extremity, particularly upper extremity sports injuries. Dr. Barth has served as a hand and wrist consultant for the Washington Capitals and Washington Wizards and is a former president of the Washington Orthopaedic Society. He is an associate clinical professor of Orthopaedics at The George Washington University and has served as the chief of Orthopaedic Surgery/Hand Surgery and vice chairman of the Department of Surgery at Sibley Memorial Hospital.
Dr. Richard W. Barth is a board-certified orthopaedic surgeon at Washington Orthopaedics & Sports Medicine. He specializes in surgery of the hand and upper extremity, particularly upper extremity sports injuries. Dr. Barth has served as a hand and wrist consultant for the Washington Capitals and Washington Wizards and is a former president of the Washington Orthopaedic Society. He is an associate clinical professor of Orthopaedics at The George Washington University and has served as the chief of Orthopaedic Surgery/Hand Surgery and vice chairman of the Department of Surgery at Sibley Memorial Hospital.
References
[i] Gilpin D, et al. Injectable collagenase Clostridium histolyticum: a new nonsurgical treatment for Dupuytren’s disease. J Hand Surg Am. Dec;35(12):2027-38.
[ii] Van Rijssen AL, Ter Linden H, Werker PM. 5-year result of randomized clinical trial in Dupuytren’s disease: percutaneous needle fasciotomy versus limited fasciectomy. Plast Reconstr Surg, 2011.
[i] Eaton C. Percutaneous fasciotomy for Dupuytren’s contracture. J Hand Surg Am. May;36(5):910-5.
[i] Benson LS. Dupuytren’s contracture. J Am Acad Orthop Surg. 1998;6:24-35.